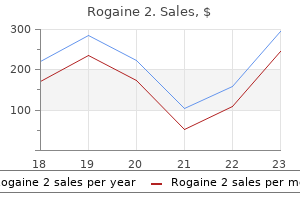
Rogaine 2 dosages: 60 ml
Rogaine 2 packs: 1 flacons, 2 flacons, 3 flacons, 4 flacons, 5 flacons, 6 flacons, 7 flacons, 8 flacons, 9 flacons, 10 flacons

Quality 60ml rogaine 2
The type 1 mesh promotes prompt ingress of fibrous connective tissue and capillaries thus encouraging tissue host ingrowth and integration permitting the mesh to anchor within the tissue. This inflammatory response wanes with time thus reducing the risk of infection (28). Slings have been extensively studied over the previous 20 years and there are numerous studies that present a considerable quantity of good high quality (level 1 and a pair of evidence) that assist the concept of a sling positioned at the degree of the mid urethra. High-quality information point out about a 7�10% failure fee for both the transobturator and the retropubic approaches, with comparable short-term remedy charges. There was no distinction in success in a 1-hour stress pad check (81% vs 90%), stress leakage (63% vs 70%), or satisfaction rates (91% vs 90%). For open colposuspension versus slings, goal cure charges at 12 months had been 79% for artificial slings versus 82% for colposuspension. For laparoscopic colposuspension versus slings, no significant distinction in patient-reported outcomes inside 12 months was proven; 80% for slings versus 74% for colposuspension (34). The biological agents assimilate into tissues over time and due to this fact sufferers want reinjections to keep ongoing symptomatic profit. Making an accurate diagnosis may be difficult and should involve invasive investigations. Conservative strategies should be trialled earlier than offering medications and or surgery. Prevalence, incidence and obstetric factors impression on female urinary incontinence in Europe: a scientific review. Fourth worldwide session on incontinence recommendations of the International Scientific Committee: analysis and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Single-incision mini-slings versus standard midurethral slings in surgical administration of female stress urinary incontinence: a meta-analysis of effectiveness and complications. Interrater reliability of filling cystometrogram interpretation in a multicenter examine. Lifestyle intervention is associated with decrease prevalence of urinary incontinence: the Diabetes Prevention Program. Effect of weight reduction on urinary incontinence in overweight and obese ladies: outcomes at 12 and 18 months. Biofeedback and behavioral therapy for the administration of female urinary incontinence. Pelvic ground muscle coaching is efficient in remedy of feminine stress urinary incontinence, but how does it work Pelvic flooring muscle coaching in remedy of female stress urinary incontinence, pelvic organ prolapse and sexual dysfunction. Stress urinary incontinence: long-term outcomes of laparoscopic Burch colposuspension. The pathophysiology of stress urinary incontinence in women and its implications for surgical remedy. Predictors of success with postoperative voiding trials after a mid urethral sling process. Three-year outcomes from a randomised trial of a retropubic mid-urethral sling versus the Miniarc single incision sling for stress urinary incontinence. Single-incision minislings versus retropubic tension-free vaginal tapes: a multicenter clinical trial. Single-incision mini-slings versus normal midurethral slings in surgical administration of female stress urinary incontinence: an updated systematic evaluate and meta-analysis of effectiveness and problems. Meta-analysis of female stress urinary incontinence therapies with adjustable single-incision mini-slings and transobturator tension-free vaginal tape surgical procedures. A prospective multicenter randomized trial of tension-free vaginal tape and colposuspension for primary urodynamic stress incontinence: two-year follow-up. Minimally invasive artificial suburethral sling operations for stress urinary incontinence in ladies: a short model Cochrane evaluation. Transurethral injection of bulking agent for the remedy of recurrent or persistent female stress urinary incontinence after mid-urethral sling. Durability of urethral bulking agent injection for feminine stress urinary incontinence: 2-year multicenter research results. They form a half of the pelvic organs and cross via the pelvic diaphragm together with the urethra and the vagina.
Buy genuine rogaine 2
Endopyelotomy: comparison of ureteroscopic retrograde and antegrade percutaneous strategies. Combination "sandwich" remedy for extensive renal calculi in 100 consecutive patients: quick, longterm and stratified results from a 10-year expertise. Long-term comparison of renal function in sufferers with solitary kidneys and/or average renal insufficiency present process extracorporeal shock wave lithotripsy or percutaneous nephrolithotomy. Morphologic and practical changes in the kidney after percutaneous nephrosto-lithotomy. The type of open procedure is set by stone measurement, configuration, and pyelocaliceal location. The process is carried out via a normal flank incision or via a dorsal lumbotomy. The proximal ureter is recognized and surrounded with a vessel loop; this aids dissection and prevents distal stone migration in the course of the procedure. The dissection is then carried proximally alongside the posterior aspect of the ureter in course of the renal pelvis. Once the pelvis is exposed posteriorly, stay sutures are placed in preparation for a transverse pyelotomy. This incision is made well away from the pelviureteric junction and carried as far laterally on the pelvis as is necessary to extract the stone beneath direct imaginative and prescient. After the stone is removed and the vessel loop is relaxed, a catheter is passed antegrade down the ureter to ensure ureteral patency. The pyelotomy is then closed in a single layer using a operating or interrupted a 4�0 absorbable suture, positioned full thickness via the renal pelvic wall. Pyelolithotomy Czerny was the first to perform removing of a stone via an incision in the renal pelvis in 1880. In basic, its use had been restricted to administration of comparatively large renal pelvic stones with or with out extension into a quantity of infundibula, but without dumbbell-shaped caliceal extensions or associated infundibular stenosis. The posterior aspect of the renal pelvis is uncovered in the identical way as that for the standard pyelolithotomy. Further publicity of the intrarenal collecting system can then be achieved using vein retractors, or specifically designed GilVernet renal sinus retractors, to elevate the posterior parenchymal lip. As described by Wulfsohn, temporary occlusion of the renal artery with native hypothermia can serve to soften the renal parenchyma and permit additional exposure of the intrarenal accumulating system. The pyelotomy is then prolonged alongside both the higher and decrease infundibula, thus creating a renal pelvic flap, which affords access to even giant calculi with early branch formation. For extra extensive stones, this approach may be combined with a easy or decrease pole nephrotomy, which is greatest reserved for sufferers with associated cortical loss and native cortical thinning. Lower pole infundibulocaliceal extensions of pelvic calculi could be managed by extending the inferior aspect of the pyelotomy incision onto the posterior renal parenchyma itself as a pyeloinfundibulotomy, immediately over the involved decrease infundibulum. Upon removing of all seen and palpable stone materials, a catheter is handed antegrade down the ureter and the intrarenal amassing system is totally irrigated. If a quantity of stones have been current, intraoperative images should be taken to exclude residual calculi. The pyelotomy incision is closed as for a standard pyelolithotomy, and an inner stent placed in chosen instances. In practice, such cases represent full, fully branched staghorn calculus with a number of dumbbell-shaped infundibulocaliceal extensions. Multiple areas of true infundibular stenosis would even be a relative indication for open operative intervention, since a slender infundibulum restricts entry to the renal pelvis. In such instances, essentially the most acceptable open operative method is usually anatrophic nephrolithotomy, as initially described by Boyce and Smith in 1967. The renal artery is quickly occluded in the course of the procedure to present a cold field, and the kidney should therefore be protected against ischaemia by cooling. Our desire is a flank approach with resection of the eleventh or twelfth rib, with medial extension of the incision to the lateral border of the rectus muscle and reflection of the peritoneum medially. Further dissection of the renal artery is accomplished until the anterior and posterior divisional branches are identified. As described by Brodel in 190123 and subsequently by Graves in 1954,24 an avascular plane exists between the junction of the blood provide to the anterior and posterior segments of the kidney. When desired, Caliceal diverticulolithotomy Caliceal diverticula are transitional epithelium-lined cavities in the renal parenchyma, which communicate with a calix or infundibulum-although that communication may not be demonstrable.
Discount rogaine 2 60ml without a prescription
Inadequate information and medical care contributes to improvement of those tumours, and applicable examination of the vulva, referral, and full-thickness biopsy of the vulval pores and skin are very important for identification of preinvasive lesions. Cervical cytology screening programmes have had an infinite impression on the incidence of cervical cancer, and the usage of vulval cytology as a screening check has been examined in quite so much of studies. Vulval most cancers epidemiology and aetiology of vulval cancer Vulval most cancers is the fourth most typical gynaecological most cancers and accounts for 6�7% of all gynaecological malignancies. Vulval most cancers is extra common in elderly ladies, with a median age at presentation of approximately sixty eight years. In the final many years, the incidence of vulval cancer has been slowly increasing (45, 46). Squamous cell carcinoma is the most common type, and accounts for 80�90% of all circumstances. Malignant melanomas, adenocarcinomas, and basal cell carcinomas are a lot less widespread. Haematogenous unfold and spread by direct extension additionally occur, however are a lot less frequent. Some sufferers present with vulval bleeding, discharge, dysuria, or a metastatic mass within the groin. This delay particularly occurs when doctors prescribe medicine with out correct visible inspection of the vulva. Several tumour characteristics are essential to document, as they could influence major treatment planning: size of the lesion, uni- or multifocality, and distance to the midline describing whether or not the tumour encroaches critical midline buildings such as the clitoris, anus, or urethra. Distance of the medial margin of tumour to the midline determines whether or not ipsi- or bilateral lymph drainage to the groins is to be expected and thereby whether or not groin treatment ought to be ipsi- or bilateral. Such information is necessary for treatment planning and for accurate pretreatment counselling of the affected person. Palpation of the groins should also be performed, as this is the primary web site of lymphogenic metastasis. The analysis of vulval cancer is made by an incision biopsy or punch biopsy for histopathological examination. For correct therapy planning the localization of the first tumour is essential. In sufferers with a number of vulval lesions, all lesions should be biopsied individually, with clear mapping of the vulva. Because vulval most cancers is such a uncommon disease, and outcome of therapy is related to expertise of the treating physicians, therapy ought to be centralized in centres by a multidisciplinary group with sufficient expertise within the treatment of this disease. Members of the staff ought to include urologists, colorectal surgeons, plastic surgeons, and radiation oncologists. The variety of lymph node metastases has been shown to have major influence on survival; a 5-year survival of greater than 90% for patients with adverse nodes, 75% for sufferers with one or two constructive nodes, 36% for sufferers with three or four positive nodes, 24% for patients with five or six optimistic nodes, and 0% for sufferers with seven or extra positive nodes (53). These results led to the incorporation of the number and measurement of lymph node metastases in the most recent staging system (56). Management of early-stage vulval cancer History of surgical therapy the cornerstone of treatment of vulval cancer patients is surgery. A current Canadian examine on patterns of care in 978 vulval most cancers patients confirmed that 85% had at least one surgical procedure, and approximately 25% received radiotherapy (57). Standard remedy for squamous cell most cancers of the vulva has modified dramatically during the last a long time. This radical method drove out easy native excision in the second half of the last century and became the usual of look after a prolonged period of time. The rationale for this strategy was the belief that prognosis is best after elective inguinofemoral lymphadenectomy compared to surveillance of the groins, despite the very fact that only about 30% of sufferers may have inguinofemoral lymph node metastases. Wound breakdown, infections, and lymphoedema have been of nice concern and sometimes resulted in prolonged hospitalization. Since then, many modifications of surgery have been proposed within the therapy of vulval most cancers patients with the purpose of all modifications to scale back morbidity of vulval most cancers therapy without compromising survival charges. Steps forward have been made with the introduction of inguinofemoral lymphadenectomy via separate groin incisions (61), replacement of radical vulvectomy by extensive local excision (62), abandonment of bilateral lymphadenectomy in lateralized tumours lower than 2 cm in measurement (63, 64), and abandonment of inguinofemoral lymphadenectomy in microinvasive tumours (<1 mm depth of invasion) (52). Due to these modifications, treatment-related morbidity has decreased, but remains to be important for sufferers undergoing inguinofemoral lymphadenectomy.
Buy 60ml rogaine 2 amex
The medical target volume consists of the first cervical tumour, upper vagina, parametria, and pelvic lymph nodes including the external and internal iliac and presacral lymph nodes. In patients with concerned pelvic nodes, the scientific goal volume could additionally be expanded to include frequent iliac nodes, and those with widespread iliac involvement might require therapy of the following echelon para-aortic lymph nodes. An important element includes shields to scale back the bowel, bladder, and femoral head dose. Role for concurrent chemotherapy and radiation Based on a sequence of five randomized trials reported in 1999, which demonstrated improved survival and acceptable toxicity, concurrent weekly cisplatin in 5 courses (at a dose of 40 mg/m2) and radiotherapy has turn into the standard of care in cervix most cancers (45). Role for radiotherapy by stage Decisions regarding optimal remedy for early-stage disease are critically dependent on a multidisciplinary discussion between gynaecological, radiation, and medical oncologists, with enter from gynaecological imaging and pathology. Definitive chemoradiotherapy is curative in ladies with cervix cancer, in part because of the mixture of exterior bean radiation with intracavitary brachytherapy, delivering a excessive native dose to the tumour whereas sparing normal tissues (46); and partly because of the elevated radiosensitivity and better outcomes related to human papillomavirus-related tumours, together with other human papillomavirus-related sites corresponding to oropharynx (47, 48). Typical therapy consists of external beam pelvic radiotherapy (45 Gy in 25 daily fractions over 5 weeks) plus concurrent weekly cisplatin chemotherapy, followed by intracavitary brachytherapy. External beam pelvic radiotherapy (45�50 Gy) plus concurrent cisplatin chemotherapy, adopted by intracavitary brachytherapy results in progression-free and total survival in 65�70%, depending on stage (52). Locally advanced/metastatic cervix most cancers Patients with regionally superior or metastatic illness are assessed for appropriate palliative treatment, which may include mixtures of chemotherapy, radiation, or no active therapy till symptoms come up. Locally recurrent tumours could additionally be appropriate for retreatment with radiation to deal with ache and bleeding (53). Postoperative radiotherapy External beam chemoradiation remedy is recommended for highrisk options following modified radical hysterectomy and pelvic lymph node dissection together with shut or optimistic surgical resection margins, the presence of capillary lymphatic invasion, and positive pelvic lymph nodes. Randomized studies have proven improved outcomes, notably with adenocarcinomas, with low charges of serious toxicity (54). Brachytherapy Intrauterine tandem applicator with vaginal colpostats or ring using high-dose rate afterloading brachytherapy is used during or following exterior radiotherapy. Typical doses are 28�30 Gy in four to 5 fractions (36�40 Gy low-dose price equivalent) of high-dose rate brachytherapy within the third to fifth week of external beam radiotherapy, relying on tumour response. Follow-up care this entails clinic visits for assessment including pelvic exam every 3�4 months for two years after completing remedy, then each 6 months to 5 years. Cervical/vaginal cytology is carried out on the discretion of the oncologist starting 1 year after finishing radiotherapy so as to avoid false-positive results because of radiation effects. Hormone substitute remedy may be thought-about for patients who had been premenopausal previous to treatment. Uterine most cancers Role for radiotherapy by stage Despite a long time of study, the role of adjuvant therapy within the treatment of endometrial cancer has been tough to define. Radiotherapy has been proven to reduce the danger of local recurrence but its effects on survival remains unclear. Several elements contribute to the uncertainty of the role of radiotherapy, including the general failure fee which is simply 15% in all newly diagnosed endometrial most cancers confined to the uterus handled with surgical procedure, resulting in a really small enchancment in prognosis with the addition of any additional remedy. Therefore, the decision to deal with with adjuvant remedy, together with radiotherapy, relies on the understanding of the chance components of recurrence, natural history of disease, the interpretation of knowledge, and the risk of issues in every particular person case. Three randomized studies (55�57) evaluated the role of adjuvant pelvic radiotherapy and found improvement in local control but no improvement in total survival with the addition of radiotherapy in intermediate-risk patients. No difference in local control or total survival between the 2 arms was found however as expected there have been more gastrointestinal and genitourinary toxicities in the arm that acquired pelvic radiotherapy, and the conclusion was that sufferers with intermediate-risk illness should be handled with vaginal brachytherapy alone. This group is best treated with pelvic radiotherapy however as seen within the earlier dialogue has a high risk of distant metastases and questions arise whether they would benefit from systemic chemotherapy as nicely. Most of these sufferers are handled with adjuvant pelvic radiotherapy together with vaginal brachytherapy. However, if the cervical invasion is known upfront and is clinically evident by bodily exam, these patients may be treated with both radical hysterectomy followed by both pelvic radiotherapy or vaginal brachytherapy depending on pathological danger elements, or preoperative pelvic radiotherapy and brachytherapy adopted by a simple hysterectomy in 4�6 weeks. Controversy and questions stay on one of the best adjuvant remedy for patients with this stage of disease. There was similar general survival within the two arms however radiotherapy delayed native relapses and chemotherapy delayed metastases. Overall, the authors felt that the combination of chemotherapy and radiation may be a better remedy. Rare tumours Vaginal most cancers Role for radiotherapy by stage Vaginal most cancers represents solely 3% of gynaecological cancers, and given its rarity management relies largely on single-institution experience and consensus tips (69). Early stage Stage 1 cancer restricted to the vagina can often be managed by resection or partial vaginectomy with postoperative radiation or chemoradiotherapy for high-risk features similar to positive margins or nodes.
Rogaine 2 60ml amex
Comparison of urodynamics between ischemic and hemorrhagic stroke patients; can we advise the category of urinary dysfunction in sufferers with cerebrovascular accident based on type of stroke Questionnaire-based assessment of pelvic organ dysfunction in multiple system atrophy. Urethro-vesical dysfunction in progressive autonomic failure with multiple system atrophy. Urinary signs and the neurological features of bladder dysfunction in multiple sclerosis. Urodynamic findings in primary progressive a number of sclerosis are associated with increased volumes of plaques and atrophy in the central nervous system. Prospective examine on the connection between infections and a quantity of sclerosis exacerbations. Testing for urinary tract colonisation before high-dose corticosteroid treatment in acute fifty three. The price effectiveness of mixed speedy checks (Multistix) in screening for urinary tract infections. Comparison of pelvic floor muscle coaching, electromyography biofeedback, and neuromuscular electrical stimulation for bladder dysfunction in people with multiple sclerosis: a randomized pilot research. Solifenacin in multiple sclerosis sufferers with overactive bladder: a potential research. Anticholinergic medicine for adult neurogenic detrusor overactivity: a systematic evaluation and meta-analysis. Efficacy of desmopressin in patients with a quantity of sclerosis affected by bladder dysfunction: a meta-analysis. Randomized controlled trial of Sativex to treat detrusor overactivity in multiple sclerosis. Botulinum-A toxin for treating detrusor hyperreflexia in spinal twine injured patients: a new alternative to anticholinergic medicine Proposed mechanism for the efficacy of injected botulinum toxin in the treatment of human detrusor overactivity. A minimally invasive technique for outpatient native anaesthetic administration of intradetrusor botulinum toxin in intractable detrusor overactivity. Botulinum toxin A detrusor injections in patients with neurogenic detrusor overactivity considerably lower the incidence of symptomatic urinary tract infections. Treatment of refractory urge urinary incontinence with sacral spinal nerve stimulation in a number of sclerosis sufferers. Lower belly pressure versus external bladder stimulation to assist bladder emptying in multiple sclerosis: a randomized controlled examine. Do alpha-blockers have a role in decrease urinary tract dysfunction in multiple sclerosis Catheter policies for administration of long run voiding problems in adults with neurogenic bladder disorders. Minimising risks of suprapubic catheter insertion (adults only): National Patient Safety Agency, 2009. Clinical consequence of sacral neuromodulation in incomplete spinal wire injured patients suffering from neurogenic lower urinary tract symptoms. Sacral neuromodulation for neurogenic decrease urinary tract dysfunction: systematic review and meta-analysis. Transcutaneous posterior tibial nerve stimulation for therapy of the overactive bladder syndrome in a quantity of sclerosis: results of a multicenter prospective examine. Prospective evaluation of laparoscopic assisted cystectomy and ileal conduit in advanced multiple sclerosis. Functional outcomes after management of end-stage neurological bladder dysfunction with ileal conduit in a eighty. In disease, if all else fails or is inappropriate, an ileal conduit urinary diversion into an exterior amassing equipment satisfies most of those standards. Indeed, for a quantity of years following its introduction by Bricker within the Fifties,1 the ileal conduit was extremely regarded as a substitute for ureterosigmoidostomy, which was the one type of salvage surgery then available for the absent or hopelessly incontinent urinary tract within the earlier part of the 20 th century. During the Sixties and Nineteen Seventies, numerous patients were treated by ileal conduit urinary diversion, principally these having a cystectomy for bladder cancer in grownup life, or for those with unexplained higher urinary tract issues as a consequence of congenital anomalies of the decrease urinary tract in childhood. These included problems that are nonetheless tough to deal with these days similar to neuropathic bladder dysfunction, and main congenital structural abnormalities similar to exstrophy/epispadias; and, extra importantly, situations that were poorly understood on the time corresponding to severe vesicoureteric reflux and posterior urethral valves, which are actually handled quite in a unique way as a result of their nature is now understood to a a lot larger degree.
Chrysanthemum leucanthemum (Ox-Eye Daisy). Rogaine 2.
- Are there safety concerns?
- How does Ox-eye Daisy work?
- Common cold, cough, bronchitis, fever, mouth and vocal cord swelling (inflammation), liver and gallbladder problems, loss of appetite, reducing spasms, increasing the amount of urine produced (diuretic), skin swelling (inflammation), wounds, and burns.
- Dosing considerations for Ox-eye Daisy.
- What is Ox-eye Daisy?
Source: https://www.rxlist.com/script/main/art.asp?articlekey=96106
Discount rogaine 2 60ml visa
Role of adjunctive medical therapy with nifedipine and deflazacort after extracorporeal shock wave lithotripsy of ureteral stones. Is there an adjunctive function of tamsulosin to extracorporeal shockwave lithotripsy for higher ureteric stones: results of an open label randomized nonplacebo managed study. Effect of alkaline citrate remedy on clearance of residual renal stone fragments after extracorporeal shock wave lithotripsy in sterile calcium and an infection nephrolithiasis sufferers. Citrate and vitamin E blunt the shock wave-induced free radical surge in an in vitro cell tradition model. Treatment of renal calculi by lithotripsy: minimizing short-term shock wave induced renal harm by using antioxidants. Stone attenuation and skin-to-stone distance on computed tomography predicts for stone fragmentation by shock wave lithotripsy. The function of mannitol in alleviating renal injury during extracorporeal shock wave lithotripsy. Preminger Introduction to intracorporeal methods of stone fragmentation the surgical administration of nephrolithiasis has undergone dramatic adjustments over the past 40 years. Developments in radiographic tools, endourologic devices, and intracorporeal lithotrites have fully modified patient care, thereby offering simpler stone comminution with a significant discount in operative morbidity compared to the open alternate options. The use of intracorporeal lithotripsy for the management of bigger ureteral and intrarenal calculi has dramatically improved. The small working channel of the semi-rigid and versatile endoscopes has restricted the dimensions and usefulness of instruments which could be passed and used for stone removing. Indeed, for bigger stones, baskets or grasping forceps are sometimes inadequate and doubtlessly dangerous to accomplish successful stone extraction. Although the choice of intracorporeal fragmentation is incessantly based on the location and composition of the stone to be handled, the experience of the clinician and availability of apparatus usually dictates this decision. The intense warmth manufacturing within the quick area surrounding the tip of the probe ends in a cavitation bubble, which produces a shock wave that radiates spherically in all instructions. These shock waves, repeated at a frequency of 50�100 per second, result in destruction of the stone. All particles have to be washed out during intraoperative irrigation, or grasped with forceps. A piezoceramic component within the handle of the sonotrode is stimulated to resonate, and this converts electrical power into ultrasound waves (23,000�27,000 Hz) that are transmitted along the hollow metal probe making a vibrating action at its tip. When the vibrating tip is brought involved with the surface of a stone, the stone may be disintegrated. The probes come in various sizes and are handed by way of the straight working channel of a inflexible endoscope. We continue to utilize ultrasound mainly for the fragmentation of huge renal calculi during percutaneous nephrolithotripsy Electrohydraulic lithotripsy the principles of electrohydraulic lithotripsy have been described and developed by a Russian engineer in 1950. The probe is made up of a central steel core and two layers of insulation with one other metallic layer between them. Upon bubble collapse, a mechanical shock wave is generated, causing stone fragmentation. This mechanism of motion is in contrast to the holmium laser, which trigger stone destruction by vaporization. Thulium laser is one other alternative that has been lately developed and tested to use in stone management. Thulium fibre laser beam diameter is eighteen, allowing easy coupling of the laser radiation into small-core optical fibres. Such small fibres have a fantastic potential use when coupled with versatile endoscopes in demanding purposes such as access to the lower pole of the kidney for lithotripsy. Further development is necessary to improve using thulium laser as a laser lithotripsy. Laser lithotripsy the event of the pulsed dye laser for fragmentation of ureteral calculi was initiated in 1986. The pulsed dye laser delivers quick, one microsecond vitality pulsations at 5�10 Hz produced from a coumarin green dye. Instantaneous fluid evaporation causes a plasma on the stone floor, leading to a extremely localized shock wave. The 504 nm wave length produced by the pulsed dye laser is selectively absorbed by the stone, however not the encompassing ureteral wall. As the power is delivered in short pulses, minimal heat is generated, once more protecting the ureteral mucosa.
Order discount rogaine 2 line
Two keep sutures are then positioned at the medial and lateral aspects of the dependent parts of the pelvis. Bring the apex of the spatulated ureter to the inferior border of the lateral renal pelvis and produce the medial portion of the ureter to the superior edge of the pelvis. Perform the anastomosis with a fantastic interrupted or running suture corresponding to 4-0 vicryl. Postoperatively, take away the urinary catheter when the drain is dry and the drain 24 hours later if there was no further drainage. Continue the medial facet of the flap incision down the ureter beyhond the obstructed phase. Rotate the apex of the flap down to the apex of the ureterotomy and close the posterior and anterior partitions with 4-0 vicryl interrupted sutures. Scardino�Prince vertical flap this has a restricted use today for relatively long areas of proximal ureteral narrowing when the ureter is situated on the medial margin of a large box-shaped extrarenal pelvis. The flap is much like the spiral, besides the base is located extra horizontally on the dependent aspect of the renal pelvis. Form the flap from straight incisions, which converge from the bottom vertically to the apex superiorly on the posterior or anterior side of the pelvis. Develop the flap with Potts scissors, rotated down, and sutured with a 4-0 vicryl interrupted to the inferior side of the ureterotomy. A number of pyeloplasty techniques were initially described, though there now appears to be consensus that a dismembered pyeloplasty represents the strategy of selection. Laparoscopic pyeloplasty is now an accepted technique, with some authors stating it should be the standard of care in skilled arms. It is contraindicated when transposition is required and pelvic reduction is required. Position the bottom of the V on the dependent medial aspect of the renal pelvis and the apex on the pelviureteric junction. Carry the incision from the apex of the flap on to the lateral side of the ureter and lengthen distally beyhond the stenosis and a quantity of other millimetres onto normal calibre ureter. Bring the apex of the pelvic flap to the apex of ureteric incision distally and suture with 4-0 vicryl. Outline the flap with a broad base situated obliquely on the dependent renal pelvis. The minimize upper leaflet of Gerota is retracted superiorly utilizing a fan retractor and the perinephric fat is swept superiorly and inferiorly to reveal the kidney. The tissue lying inferior to the lower pole is then dissected carefully by blunt dissection, revealing the renal pelvis and ureter. The similar steps as per the transperitoneal strategy are followed at this stage with the same postoperative care. Prophylactic heparinization: unfractionated heparin 5,000 worldwide units twice a day or fractionated heparin once a day until discharge. We prefer to do that as a last verify for stones and strictures, as this can alter the surgery required. The stent could be placed antegrade during laparoscopy, but we do it at cystoscopy to make sure of its place and help in ureteric identification in troublesome instances in the course of the laparoscopic pyeloplasty. The stent is 28 Fr as this permits the J on the renal end to lie nicely above the anastomosis and not doubtlessly cantilever on it, resulting in urine leak and loosening of sutures. The stent can be placed or modified (if one has been placed previously) during the laparoscopic procedure being placed in an antegrade direction over a guidewire utilizing the superior port Catheterize patient-12�14 Ch catheter Transperitoneal and retroperitoneal approaches: As per laparoscopic easy nephrectomy Outcomes and issues Complication charges are low at 5%. Success rates primarily based on symptoms and renograms postoperatively are round 94%, comparable with open pyeloplasty results. Mean duration of surgery is 2 and a half hours and imply hospital keep is three days. These results are all comparable with open pyeloplasty and positively present a greater cosmetic outcome.
Order cheap rogaine 2 online
The function of post-operative radiation remedy for endometrial cancer: government summary of an American Society for Radiation Oncology proof based mostly guideline. Definitive radiotherapy in the administration of isolated vaginal recurrences of endometrial most cancers. Definitive radiotherapy for sufferers with isolated vaginal recurrence of endometrial carcinoma after hysterectomy. Carcinoma of the vagina-experience on the Princess Margaret Hospital (1974�1989). Neoadjuvant chemotherapy adopted by radical surgical procedure in sufferers affected by vaginal carcinoma. Surgical-pathologic variables predictive of local recurrence in squamous cell carcinoma of the vulva. Consensus recommendations for radiotherapy contouring and remedy of vulvar carcinoma. Low-stage ovarian clear cell carcinoma: population-based outcomes in British Columbia, Canada, with proof for a survival benefit on account of irradiation. Early-stage endometrioid ovarian carcinoma: population-based outcomes in British Columbia. Histotype predicts the curative potential of radiotherapy: the example of ovarian cancers. Revisiting the role of radiation treatment for non-serous subtypes of epithelial ovarian cancer. With that in mind, it represents a primary tenet of care for all sufferers, particularly these with ailments that result in vital loss of quality of life and performance. While this chapter focuses more on oncological palliative care, the tenets of palliative care and the research about symptom administration can extend to the care of girls with chronic circumstances such as continual pelvic pain, severe endometriosis, interstitial cystitis, untreatable pelvic prolapse, and other circumstances. Palliative care, then, can be a magnet for fatal and non-fatal ailments, and may and should be offered to handle diminished quality-of-life issues as a part of ongoing treatment of a illness course of, not simply at the end of life. Interdisciplinary care Effective palliative care requires a team-usually a physician, nurse, social worker, and others as needed, including dieticians, occupational therapists, physical therapists, and therapeutic therapeutic massage. Use of the creative arts and music, non secular support, psychologists, pain specialists, and disease specialists should all be added to the mix of carers. Different communities use different healthcare providers, such as conventional healers, herbalists, acupuncture, and Ayurvedic medication (among many others), and relationships with these various groups of healers ought to be pursued and respected. Not all settings could have all the elements which are needed, but the broader the perspectives and support that may be brought to bear, the higher the last word palliation of symptoms and support for quality of life. Communication with sufferers and families and coordination of care are different cornerstones of the therapeutic relationship that underpins palliative care. Care for the dying or these Pain management trade-offs Pain is essentially the most frequent symptom for cancer sufferers and distressing to all, together with caregivers. Caregivers typically make assumptions about what the aim of ache control is for a affected person, without participating the affected person in that dialogue. Some could also be willing to tolerate slightly more ache so as to be extra active with family, or may be illiberal of a loss of sensation or loss of bladder or bowel operate that might include full resolution of pain with blocks or different types of ache management. Goals could change as sufferers obtain the time they needed or the psychological or spiritual decision desired and now not want the same clarity of mentation. So particular conversations that clarify the level of pain management desired, the extent of alertness, and selections about which unwanted effects are acceptable or not are the basis of creating a ache management plan for each particular person affected person. Baseline ache management We know that pain may be managed in the majority (>90%) of sufferers (5). In addition, well-trained patients can self-manage their ache with good control (6). Every setting-home, hospital, and hospice- ought to have techniques of care that involve sufferers and households in reassessing and adjusting ache administration as circumstances change (7). Broadening availability of oral, subcutaneous, transdermal, and sublingual narcotic choices allows good-quality home-based analgesia. Intravenous or intramuscular injections are greatest avoided if home-based remedy is being carried out. Home-based therapy has other challenges including the necessity for a caregiver who can perform ache assessment, how pain evaluation is carried out, compliance with the regimen, and issues of hesitance to report pain and lack of schooling (11).
References
- TAIM Study, Wassertheil-Smoller S, et al. The Trial of Antihypertensive Interventions and Management (TAIM) Study. Final results with regard to blood pressure, cardiovascular risk and quality of life. Am J Hypertens 1992;5:37-44.
- Clifton GD, Branson P, Kelly HJ, et al: Comparison of NS and heparin solutions for maintenance of arterial catheter patency. Heart Lung 20:115, 1991.
- Ozaras R, Yemisen M, Mete B, et al: Acrocyancosis developed with amphotericin B deoxycholate but not amphotericin B lipid complex, Mycoses 50:242, 2007.
- Lee RP, Teichgraeber JF, Baumgartner JE, et al. Long-term treatment effectiveness of molding helmet therapy in the correction of posterior deformational plagiocephaly: a five-year follow-up. Cleft Palate Craniofac J 2008;45:240-245.
- Zonta M, Angulo M, Gobbo S, et al. Neuron-to-astrocyte signaling is central to the dynamic control of brain microcirculation. Nat Neurosci 2003;6:43-50.
- Singer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801- 810.
- Sokoloff MC, Goldberg LS, Pearson CM. Treatment of corticosteroid- resistant polymyositis with methotrexate. Lancet. 1971;1(7688):14-16.
- Bartlett JG: Clinical practice. Antibiotic-associated diarrhea, N Engl J Med 346:334n339, 2002.